Quantitative EEG (qEEG)
What is a qEEG (sometimes called a “Q”)?
A quantitative EEG (qEEG) is an EEG brain map. Compared to an MRI, it’s less expensive and provides much more specific information about cortical timing. The brain is incredibly fast, and even minuscule differences in timing in a brain area can have profound functional implications.
In very simple terms, a qEEG is a computer analysis of the EEG data. It typically uses 19 or more channels of simultaneous EEG recording under specific recording conditions.
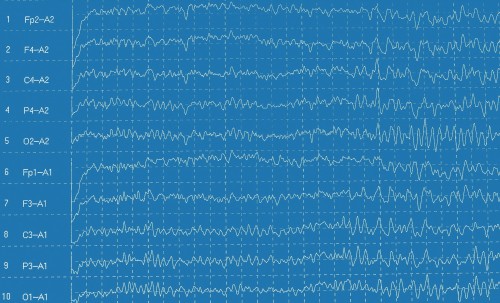
An example of raw data of a qEEG.
This EEG data is compared against a reference database of other people’s EEGs. The analysis identifies and highlights variations from the norm (average). For instance, the qEEG report could show brain areas where there is too much or too little EEG activity compared to the norm. It could also show which areas are not communicating well with other areas. Excessive EEG activity or poor communication typically correlate with lower brain efficiency.
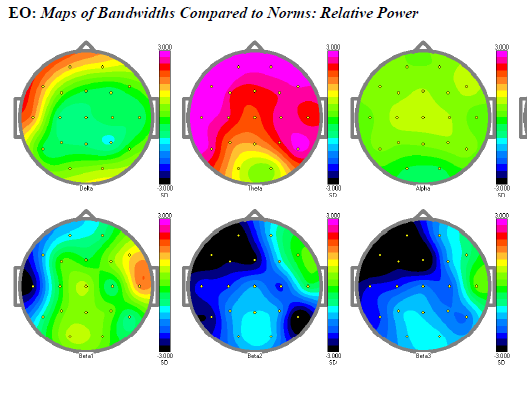
An example from a qEEG report.
A great deal of effort goes into creating these averages – also called normal databases. It involves careful screening to exclude people with a history of problems like attention, depression, anxiety, learning problems, etc. A wide age range must also be represented.
How important is combining a qEEG with neurofeedback?
qEEG reports, along with the EEG record, help provide more information about a client’s brain. That information can help a trained professional better target neurofeedback training.
At the major professional conference in the field, there’s a large effort to increase education and tools that make qEEG-based training more accessible. It provides a basis for evidence-based intervention at a time when the FDA is increasingly interested in evidence-based medicine. There’s an increasing consensus that the qEEG, combined with analyzing the EEG, often provides valuable information about an individual’s brain problem and can speed the results and efficacy of neurofeedback training.
Others in the field don’t agree about the need to use qEEG reports. For example, there are some camps in the field who promote neurofeedback training as a tool for changing a complex dynamic system. They descibe the brain as a self-organizing system. They contend that the type of neurofeedback training they offer achieves equivalent success without requiring a qEEG. They may use only a small number of sites to train with neurofeedback. They claim that adding in a qEEG does not improve success.
 More study comparing all the approaches needs to be done. Other providers do what is sometimes referred to as mini-qEEGs (which are sometimes incorrectly described as qEEGs). They tend to use certain ratios or data relationships as guidelines to target training based on limited data and a limited number of sites. Other models target training-specific brain systems that often correlate with symptoms. It seems clear that more information about a client’s brain can help with training.
More study comparing all the approaches needs to be done. Other providers do what is sometimes referred to as mini-qEEGs (which are sometimes incorrectly described as qEEGs). They tend to use certain ratios or data relationships as guidelines to target training based on limited data and a limited number of sites. Other models target training-specific brain systems that often correlate with symptoms. It seems clear that more information about a client’s brain can help with training.
Some clinicians suggest that not every client needs to spend the money on a qEEG. Certain types of problems may respond to training certain regions of the brain. Other clinicians point out that problems may be missed without screening the individual via a qEEG. Since qEEG reports can be somewhat costly, the choice of doing the test should be discussed between the client and clinician.
Even within the field, different experts may interpret the information differently. The brain is incredibly complex, and information about neuroscience is always evolving. Think of a qEEG or an EEG like a blood test. When the clinician gets a blood test back, it provides information, but it’s not always clear exactly how to best tackle the problem. The qEEG is similar. It provides clues, but the experience and knowledge of the clinician will affect how he or she uses the information.
Can a clinician use a qEEG without specific training or experience?
There’s a pretty big learning curve to interpreting and applying qEEG information. Some clinicians choose to start by learning both the qEEG and neurofeedback at one time. Others find that they either start without the qEEG using other models of training, or they rely on experts who provide a service analyzing and interpreting the qEEG, as well as sharing how to use it with neurofeedback clients. These services allow newer clinicians to start using qEEG reports relatively quickly and with a smaller learning curve. It’s probably reasonable to say that the more education a clinician has, the easier it is to effectively use the information in the report.
Can qEEG’s improve neurofeedback training?
When you talk with clinicians who have a lot of experience using qEEG’s, they say the report often helps training decisions and improves outcomes. The qEEG gives more clarity about what’s happening in the brain. When clinicians have not developed much expertise with a qEEG, they often say they don’t get consistent help from the information. Some experienced clinicians also say they’ve achieved equal success without using a qEEG. There are some experienced clinicians who fall in the middle – they feel a qEEG can be very helpful, but that they know enough based on other information that it’s not always needed.
Is it important to combine the qEEG report with clinical data, or can I work from the EEG itself?
 Many experienced clinicians and qEEG providers feel it’s very important to correlate the EEG and qEEG report. The qEEG is a statistical report. If it’s accurate, it should have some correlation to the client’s presenting symptoms – from a neurophysiological perspective.
Many experienced clinicians and qEEG providers feel it’s very important to correlate the EEG and qEEG report. The qEEG is a statistical report. If it’s accurate, it should have some correlation to the client’s presenting symptoms – from a neurophysiological perspective.
For example, if they have bad problems with organization and their report shows excessive slowing prefrontally (executive function), the two correlate nicely. However with the same problem, if there were no problems in the qEEG except at the right temporal lobe, there may need to be careful interpretation of the symptoms the client is reporting. If the client reports a problem and the qEEG report doesn’t correlate well, this is also valuable clinically.
Is there clinical information in the EEG that isn’t in the qEEG?
Yes. The qEEG is an average of the EEG over time. There are details or events in the EEG that may get lost or averaged out in the qEEG. Both are important to look at. Certain spikes, unusual periodic bursts in the EEG, or unusual wave forms may all be significant, but not show up in the qEEG report itself.
Do I need to buy special qEEG equipment?
You either need special equipment or you need to send your client to a location that records the EEG for you. Though hospitals and neurologists have EEG recording equipment, it’s rare that they are compatible with the requirements needed to run neurofeedback-oriented qEEG’s. There are a variety of equipment options, each with pros and cons. Some services may even provide you the equipment for free if you pay for several of their qEEG reports monthly. You may also be able to find a local EEG tech to do the recordings but not to interpret the report.
How many qEEG’s do I need to justify my own equipment and software?
If you average 2-3 qEEG’s a month, it probably justifies a 19+ channel digital EEG machine ($200-350 leased a month or $7-12k to purchase). Once people have a qEEG machine, they usually end up offering it to more of their clients. It can be a useful tool for many clients who find the concept of getting a brain map credible and tangible information.
Should I use a qEEG service or analyze the EEG data myself?
 If you choose to get equipment and learn to use qEEG reports, you can take courses to help you learn how to do it with a good instructor. Even then, you’ll need some mentoring to gain skill and be more productive. Of course, that’s true with learning neurofeedback anyway.
If you choose to get equipment and learn to use qEEG reports, you can take courses to help you learn how to do it with a good instructor. Even then, you’ll need some mentoring to gain skill and be more productive. Of course, that’s true with learning neurofeedback anyway.
Many professionals find someone experienced in neurofeedback to help mentor them and speed up the learning curve after their initial courses. Some start by learning neurofeedback only. There are those who feel it’s such an important tool that they should start with it. Others find it’s a big learning curve.
It is faster to find an individual or service that specializes in helping clinicians interpret the qEEG report and make neurofeedback recommendations based on the findings. Be extremely cautious about the service or people you work with. Many people who purchase equipment and the software still get help in interpreting reports as part of the learning process.
If you use someone to help interpret the qEEG, how does that work?
First, you need to get the EEG data recorded, which can be done in your office or by sending the client to another office that has the equipment. You then send the EEG files digitally via the internet. Once the files are received, the person interpreting it will clean up the EEG data, analyze it, and produce a report.
Reports vary widely depending on the individual or service providing them. An email version of the final report will be sent to you in full color and/or sent as a printed “hard copy”. Getting a neurofeedback recommendation requires you to use someone very knowledgeable in both neurofeedback and qEEGs.
Is there insurance reimbursement?
Two main billing codes apply: 95816 for recording the EEG and 95957 for analysis of the EEG. The professional interpretations are billed with the same codes, adding the trailer “–26”. Several psychologists and licensed therapists have reported success with insurance reimbursement with billing code 95957 without an MD. One therapist going through a physician for billing reported high reimbursement success.
Do qEEG’s improve client compliance?
Several clinicians think a qEEG adds credibility and has improved client motivation and compliance to help get them started and stick with their neurofeedback program. They say clients often feel relief when they see the pictures, and that it makes their problem more real.
If you don’t give a qEEG to everyone, who should it be recommended to?
This is a judgment call, but here are some indications to seriously consider it:
- TBI/Stroke/Head injury/Concussion
- Rage disorders
- Seizures
- Long difficult psychiatric/medical history with little response to many medications
- Suicidal depression
- Existing neurofeedback client who is making little or no progress within 8-15 sessions
How important is the database?
There are major differences in the various normative databases that exist. You can choose from SKIL, NX-Link, Neuro-rep, and others. Each has it’s pros and cons. There is no perfect database. Ultimately, it may be more important to find a consultant and let him or her help you choose.
Are there good courses available for learning the qEEG?
 There are many courses for learning the qEEG. They are a bit difficult to find, not provided consistently, and you’re likely to need several in order to really get up to speed. We hope to help provide more ready access to qEEG courses – a step 1, 2, 3 set of courses that are more consistently provided. One course isn’t enough. There are courses offered at conferences and by some individual organizations.
There are many courses for learning the qEEG. They are a bit difficult to find, not provided consistently, and you’re likely to need several in order to really get up to speed. We hope to help provide more ready access to qEEG courses – a step 1, 2, 3 set of courses that are more consistently provided. One course isn’t enough. There are courses offered at conferences and by some individual organizations.
Because of the learning curve, taking any or all of these course may be useful, though not always cost-effective. Again, it may be useful to receive consulting to help identify the best fit (course, equipment, mentor) for an individual practice.
Are there criteria for choosing a qEEG service provider or individual knowledgeable in qEEG’s?
- Ask questions about their knowledge and experience in both qEEG’s and neurofeedback.
- Talk to several neurofeedback users they’ve worked with to see how successful the interactions are. There is no substitute for talking to users.
- Don’t pick someone because they are close. Expertise is more valuable than proximity.
- Try them out with one or two clients to see if it’s a good fit.
- Find out how you can use their recommendations. Look at some of their reports, and discuss their approach. Since there are different approaches and models in neurofeedback, how well do their recommendations fit your training model? How much protocol expertise and savvy do they have?
Does a qEEG ever show a client as normal when he or she isn’t normal?
Yes, it can happen. Clinicians with head-injured or other severely dysfunctional clients sometimes receive qEEG reports that appear to be within the range of normal variation, meaning it may look “OK” when the person is clearly not okay. This also depends on the skill of the individual reading the report and their ability to identify subtle problems.
Like medical tests, a qEEG won’t always help. The more experienced the reader, the more likely you are to identify clues. You may have two different people read the same qEEG report and come up with different information. Interpreting qEEG data is still both a science and an art.
What does “training to the Q” (qEEG) mean?
In the strictest sense, it means that if your qEEG varies from the normal EEG database, you train the areas that vary from the norms until they are normal. The problem is the qEEG doesn’t actually tell you the right training strategy for targeting the problem identified. To use it, you need knowledge of how to apply neurofeedback.
For example, if the qEEG showed excessive low frequency at Fp2 (right prefrontal), do you train down the low frequency, train up a higher frequency, do both, or neither? Could that person’s brain respond better by training another site? Someone who’s done much neurofeedback knows that training FP2 by itself at faster frequencies has real potential for problems.
How can problems recording the EEG affect qEEG reports?
The qEEG report may have problems as a result of (1) artifact, (2) problems staying alert during the qEEG, or (3) use of medications or over-the-counter remedies that were not disclosed to the clinician. Without a very experienced EEG reader/clinician, these problems can affect the qEEG report inappropriately.
For example, let’s say someone gets sleepy while having their EEG recorded. If that’s not clearly identified (which requires both experience and careful diligence to the raw EEG), the report could show excessive slow activity when in fact, the client was just tired.
The problem with statistics: Can the same data yield different recommendations?
A qEEG is a statistically-based report. When you compare an individual’s data against an averaged “normal” database, any variation in an individual’s data that is less than 2.0 standard deviation is not considered statistically significant in traditional neurometric analysis. But when there are thousands of calculations, it’s not that unusual for several of the qEEG report numbers to be high or low. This can be a statistical anomaly. No one number in the report, even if it’s way off norms, by itself identifies a problem.
What are some other reasons neurofeedback recommendations can vary based on a qEEG?
EXAMPLE: Let’s say the qEEG identifies a coherence problem. Some recommendations could include coherence training between the offending sites. However, a contrary opinion suggests that training the primary site with unipolar training, such as training F3 with 15-18 Hz (to get it regulating itself properly), can often eliminate the coherence problem without the need to train coherence directly. Could there be times where coherence training may be needed? Yes. Is there one right answer? Probably not.
Are qEEG’s consistent from day to day? Can there be a lot of variability?
The qEEG has been studied for years. Many studies document the EEG measurement to be very consistent, such that if you have seen one person’s qEEG today, and you saw the same person tested one week later, both could usually be easily identified as belonging to the same person by an experienced EEG analyst. The reliability of the process needs to be assured by good technique such as proper sampling of the EEG and elimination of state changes such as drowsiness or medication changes.
We do see changes over time as neurofeedback treatment continues and the brain learns new, healthier patterns. A qEEG done after the third session will likely look different than a qEEG done after the 40th session.
Does a qEEG compare to other brain scans, such as MRI, SPECT scans, CAT scans?
This topic probably requires a longer discussion of Amen’s work with SPECT scans and how this work compares with qEEG. The very short answer is that both can be helpful to neurofeedback protocol recommendation. However, a qEEG is potentially better for development of neurofeedback protocols at this time due to specific timing features in the recommendations. A SPECT scan, for example, may provide better indicators on perfusion, particularly subcortically, but not necessarily timing.
